Answer Question Screen
- Clean multiple-choice interface with progress bar.
- Mark for review feature.
- Matches real test pacing.
Strike while the savings are hot! Use promo code FlashSale at checkout for 12% off any Exam Edge test or bundle. Hurry—the clock is ticking!

** All Prices are in US Dollars (USD) **
Understanding the exact breakdown of the BCEN Certified Emergency Nurse test will help you know what to expect and how to most effectively prepare. The BCEN Certified Emergency Nurse has 175 multiple-choice questions . The exam will be broken down into the sections below:
| BCEN Certified Emergency Nurse Exam Blueprint | ||
|---|---|---|
| Domain Name | % | Number of Questions |
| Cardiovascular Emergencies | 12.7 % | 22 |
| Respiratory Emergencies | 12.0 % | 21 |
| Neurological Emergencies | 12.0 % | 21 |
| Gastrointestinal - Genitourinary - Gynecology & Obstetrical Emergencies | 12.0 % | 21 |
| Mental Health Emergencies | 7.3 % | 13 |
| Medical Emergencies | 9.3 % | 16 |
| Musculoskeletal & Wound Emergencies | 8.7% | 15 |
| Maxillofacial & Ocular Emergencies | 7.3 % | 13 |
| Environment & Toxicology Emergencies Communicable Diseases | 9.3% | 16 |
| Professional Issues | 9.3 % | 16 |
Everything you need to prepare with confidence—without wasting a minute.
Timed, No Time Limit, or Explanation mode.
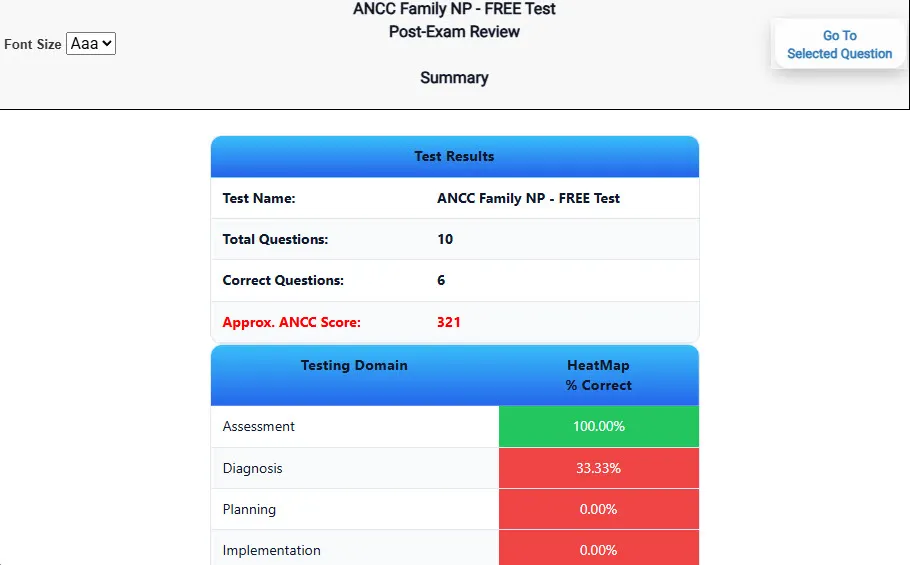
Heatmaps and scaled scores highlight weak areas.
Concise explanations emphasize key concepts.
Matches the feel of the actual exam environment.
Clean layout reduces cognitive load.
Web-based access 24/7 on any device.
Our practice tests are built specifically for the BCEN Certified Emergency Nurse exam — every question mirrors the real topics, format, and difficulty so you're studying exactly what matters.
We match the per-question time limits and pressure of the actual BCEN exam, so test day feels familiar and stress-free.
You'll have more than enough material to master every BCEN Certified Emergency Nurse concept — no repeats, no fluff.
Ordering 5 practice exams costs less than retaking the BCEN Certified Emergency Nurse exam after a failure. One low fee could save you both time and money.
Need to step away mid-exam? Pick up right where you left off — with your remaining time intact.
See your raw score and an estimated BCEN Certified Emergency Nurse score immediately after finishing each practice test.
Review correct and incorrect answers with clear, step-by-step explanations so you truly understand each topic.
We're fully accredited by the Better Business Bureau and uphold the highest standards of trust and transparency.
No software to install. Access your BCEN Certified Emergency Nurse practice exams 24/7 from any computer or mobile device.
Need extra help? Our specialized tutors are highly qualified and ready to support your BCEN exam prep.
Preparing for your upcoming BCEN Certified Emergency Nurse (CEN) Certification Exam can feel overwhelming — but the right practice makes all the difference. Exam Edge gives you the tools, structure, and confidence to pass on your first try. Our online practice exams are built to match the real BCEN Certified Emergency Nurse exam in content, format, and difficulty.
These BCEN Certified Emergency Nurse practice exams are designed to simulate the real testing experience by matching question types, timing, and difficulty level. This approach helps you get comfortable not just with the exam content, but also with the testing environment, so you walk into your exam day focused and confident.
“ The questions on this application aren't really what the CPEN covers. A lot of obscure stuff. Also, the questions are too easy (like I said, not CPEN-quality.) Skip this app.
Here is a list of alternative names used for this exam.

